


OESOPHAGEAL CANCER
OESOPHAGEAL CANCER (CANCER OF THE OESOPHAGUS)
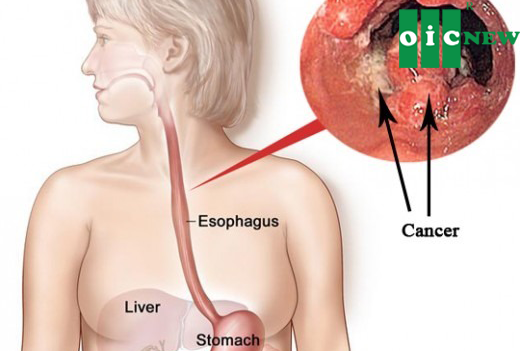
Oesophageal cancer, or cancer of the oesophagus, may also be referred to as cancer of the gullet or food pipe. The oesophagus is a muscular tube measuring 20-25 cm (8-10 in) long and 2-3 cm (0.75-1.25 in) wide that serves as a conduit for moving food and drink from the mouth to the stomach. Two major types of oesophageal cancers exist, as follows:
- Squamous cell carcinoma arises from the epithelial cells that line the oesophagus.
- Adenocarcinoma arises from the oesophageal glands or within a segment ofBarrett's oesophagus.
Most tumours occur in the lower oesophagus.
- 40% occur in the lowest third.
- 45% occur in the middle third.
- 15% occur in the upper third.
Risk factors
Risk factors for oesophageal cancer include alcohol abuse, smoking, obesity, poordiet and nutrition and age – being over 55. Long-term exposure to some chemicals may play a role, as does having the condition Barrett's oesophagus or gastro-oesophageal reflux disease (GORD).
Cancer of the oesophagus symptoms
Symptoms of oesophageal cancer usually do not show up until the disease has reached an advanced stage.
The most common symptom is difficulty swallowing (dysphagia).
- Initially, swallowing solids is difficult.
- Over time, even swallowing liquids becomes difficult.
The following symptoms may accompany cancer of the oesophagus. Any of these symptoms are indications of advanced disease and should be considered as a sign to get medical attention.
- Weight loss
- Central chest pain
- Pain upon swallowing
- Vomiting
- Chronic cough
- Symptoms of gastrointestinal bleeding
- Black stools
- Vomiting blood or material that looks like coffee grounds
Diagnosis of cancer of the oesophagus
The best diagnosis is based on findings from an endoscopic examination of the oesophagus.
- The doctor administers a topical anaesthetic to the throat to suppress the gag reflex. Doctors frequently give intravenous (IV) sedation just before the procedure.
- The doctor then inserts an endoscope into the oesophagus. An endoscope is a thin, flexible plastic tube that contains fibre optic bundles.
- Using a tiny camera in the endoscope, the doctor searches the surface of the oesophagus for areas of concern.
Doctors define oesophageal tumours in terms of their size and location.
- Stage 1 - Cancer limited to the top layers of the cell lining
- Stage 2 - Cancer extending deeper into muscle layers of the oesophagus and may have spread into adjacent lymph nodes
- Stage 3 - Cancer has spread through the wall of the oesophagus and into adjacent tissues and lymph nodes
- Stage 4 - Cancer has spread to other parts of the body such as the liver or lungs
The doctor can take biopsies to confirm whether the abnormality is a cancer and to determine its type. Upper gastrointestinal (GI) barium contrast studies help the doctor to detect cancers but may fail to detect small tumours more easily seen through endoscopy.
Once the presence of cancer has been confirmed, the doctor tries to determine the spread of the malignancy beyond the oesophagus. Doctors may use the following imaging tests:
- CT scan of the chest and abdomen
- Chest x-ray film
- Nuclear bone scans
Cancer of the oesophagus treatment
Treatment for oesophageal cancer depends on the results of tests and your underlying health. People with advanced heart or lung disease may not be candidates for aggressive treatment. In many cases, the oesophageal cancer has advanced too far for any available treatment to work. In these cases, the doctor considers the following procedures:
- Placing a metal or plastic tube ( stent) in the oesophagus to allow passage of food and liquids
- Radiotherapy
- Photodynamic therapy
- Widening the oesophagus or laser destruction of the oesophageal tumour
In otherwise healthy people with localised disease, surgery may offer the best chance of long-term survival.
- Surgery involves removing the diseased portion of the oesophagus and connecting the remaining portion to the stomach.
- Pre-operative chemotherapy and radiotherapy often accompany surgery.
Oesophageal cancer: Prognosis
When the oesophageal cancer has spread to organs beyond the oesophagus, long-term survival is uncommon. The chance of recovery improves when doctors detect the cancer at an early stage. But in most cases, long-term survival remains below 30%. Once cancer invades the muscle layer of the oesophagus, most people already have developed widespread cancer. For these people, cancers invariably come back following surgical removal. Few people survive long-term.
Following completion of therapy, whether with surgery, radiotherapy, chemotherapy, or a combination of these, the patient needs regular follow-up endoscopic examinations as well as repeat CT scans of the chest and abdomen. Often, people who undergo surgery of their oesophagus develop significant narrowing at the site of the surgery. They require frequent oesophageal dilatations or insertion of stents.
Oesophageal cancer: Prevention
Reducing use of alcohol can reduce the frequency of squamous cell carcinoma of the oesophagus. According to Cancer Research UK, if you smoke and drink a lot, your risk of squamous cell carcinoma is much greater. The combined risk is greater than the risk of just smoking or the risk of just drinking. Not smoking reduces the risk of both squamous and adenocarcinoma of the oesophagus. Maintaining a healthy weight also may reduce the risk of developing oesophageal cancer.
Adenocarcinoma of the oesophagus is a frequent complication in Barrett's oesophagus, which may be found in up to 20% of people with symptoms of gastroesophageal reflux disease (GORD). People with GORD may be advised to should undergo screening with endoscopy.
People with Barrett's oesophagus should have regular endoscopic tests to detect precancerous changes of the oesophageal lining. They also require tight control of the symptoms of gastro-oesophageal reflux, which may include dietary and lifestyle changes as well as medications and possible surgery, to prevent progression of Barrett's oesophagus.
Source: http://www.webmd.boots.com/cancer/cancer-of-the-oesophagus?page=2
Liquid Nano Curcumin OIC is available in large pharmacies in Vietnam. Please contact our Customer Service Hotline at 1900636913 or access DISTRIBUTION CHANNELS to receive information of the nearest pharmacy.
The product is not a medicine and cannot replace medicines

The most-read articles
- HEALTHCARE AND THE USE OF NANOTECHNOLOGY IN MEDICAL APPLICATIONS
- HOME REMEDIES FOR A STOMACH ULCER
- GALLBLADDER DISEASE
- TRY TURMERIC FOR QUICK RELIEF FROM A SORE THROAT
- Pycnogenol
- THE BEST THINGS TO KNOW ABOUT THE ALOE VERA PLANT
- RESULTS OF SCIENTIFIC RESEARCH ON LIQUID NANO CURCUMIN OIC
- NANOTECHNOLOGY IN COSMETICS
- OESOPHAGEAL CANCER
- GOUT: SYMPTOMS, CAUSES, AND TREATMENT
Send your question